Background
Severe Fever with Thrombocytopenia Syndrome (SFTS) is a tick-borne zoonotic infectious disease first discovered in China in 2009. It primarily spreads in East Asia, with China, Japan, and South Korea being the most affected countries. In 2017, the WHO included this disease in the list of priority diseases under the Research and Development Blueprint, identifying SFTS as an infectious disease that requires urgent attention.
Numerous epidemiological studies have reported differences in clinical manifestations and mortality rates corresponding to different viral genotypes. However, there is currently no unified genotyping system. The viral strains and numbers used, clustering methods employed, and naming conventions adopted differ among various genotyping systems. The DS genotyping system not only clarifies the relationship with previously common genotyping systems, enabling horizontal comparison between different genotyping methods but also facilitates research. Our developed website serves as a unified and communicative tool, allowing researchers to quickly obtain genotyping results by uploading genetic sequences from different regions, significantly improving research efficiency.
About SFTS
-
Pathogen
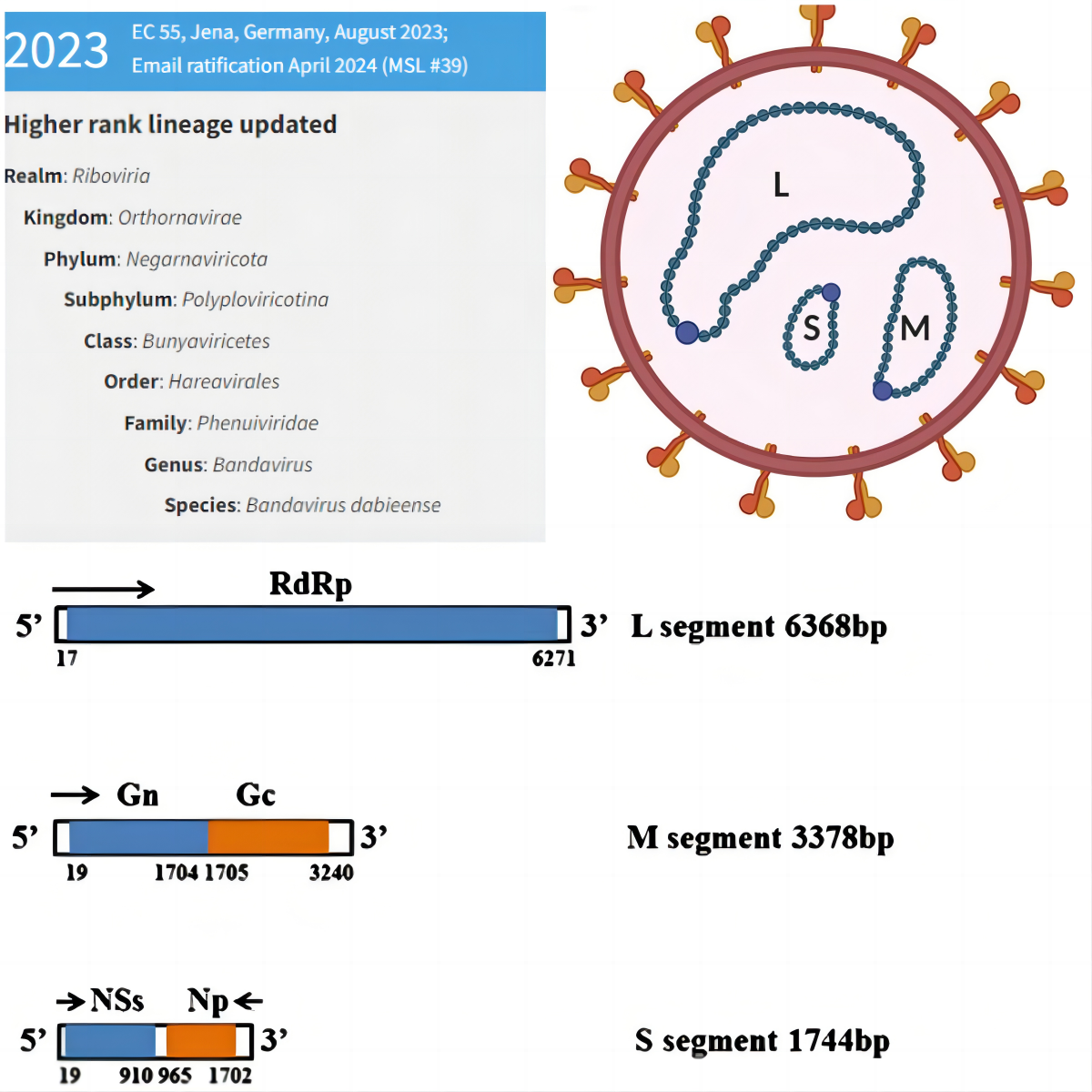
The pathogen of SFTS is Bandavirus dabieense (DBV), formerly known as severe fever with thrombocytopenia syndrome virus (SFTSV). In the 2023 ICTV classification, it is categorized under Bunyaviricetes (class), Hareavirales (order), Phenuiviridae (family), Bandavirus (genus), and Bandavirus dabieense (species). DBV is a segmented RNA virus with high genetic variability and adaptability.
-
Virus Structure
DBV is spherical and enveloped, with three segments of varying lengths: large (L), medium (M), and small (S): The L segment comprises 6368 nucleotides, primarily encoding RNA-dependent RNA polymerase, which is responsible for RNA replication and mRNA synthesis; The M segment consists of 3378 nucleotides, mainly encoding the Gn and Gc glycoproteins, which are responsible for binding the virus to host cell surface receptors and invading the cell through membrane fusion; The S segment includes 1744 nucleotides, encoding non-structural protein NS and nucleocapsid protein NP, which are associated with viral immune evasion.
-
Population Distribution
The primary occupation of SFTS cases is farming, accounting for 85.82%, followed by household duties and unemployment, accounting for 6.99%. The age group primarily affected is between 50 and 74 years, accounting for 69.46%. From 2011 to 2021, the reported male-to-female ratio of SFTS cases in China was 0.89:1. The cumulative incidence rate was slightly higher in females (1.491 per 100,000) than in males (1.266 per 100,000), with a statistically significant difference (χ²=126.57, P < 0.001). The male-to-female ratio of SFTS death cases was 1.11:1. The cumulative fatality rate was slightly higher in males (5.70%) than in females (4.58%), also showing a statistically significant difference (χ²=12.25, P < 0.001)[1]。
-
Seasonal Distribution
The number of cases starts to gradually increase in March, reaching a peak in May, and then begins to decline. The onset dates for 96.79% (8,551/8,835) of the cases are distributed between April and October, with 57.36% (5,068/8,835) of the cases occurring between May and July. The earliest death cases appeared in March, increasing with the number of cases, and are mainly distributed from May to July (63.58%, 302/475)[2]。
Clinical Characteristics
The main clinical symptoms and signs of SFTS include acute high fever, thrombocytopenia, leukopenia, elevated serum liver enzyme levels, gastrointestinal symptoms, and multi-organ failure [3]. Severe cases may also present with neurological symptoms such as altered mental status [4].
Initial stage
Initial stage (or febrile phase): Also known as the fever phase. The onset is abrupt with high fever, typically ranging from 38 to 40°C. Symptoms include fatigue, loss of appetite, nausea, vomiting, and in some cases, muscle aches and diarrhea. A few patients may experience apathy. Physical examination often reveals swollen superficial lymph nodes in the groin, neck, or armpits, accompanied by tenderness. In more severe cases, there may be local redness, swelling, heat, and pronounced pain.
Critical stage
Critical stage (or multi-organ dysfunction phase): Also known as the critical phase. It can overlap with the febrile phase and is characterized by sustained high fever, potentially with remittent fever, extreme fatigue, and exacerbated gastrointestinal symptoms. Some patients may exhibit involuntary tremors in the jaw or limbs with increased muscle tone. Severe cases may present with skin petechiae, gastrointestinal bleeding, pulmonary hemorrhage, restlessness, delirium, and in extreme cases, seizures, coma, and death due to circulatory failure, respiratory failure, hemorrhage, etc.
Recovery phase
During this phase, the fever subsides, symptoms gradually improve, and normal body temperature returns. Recovery typically occurs around two weeks, but for those with complications, the course of illness may be prolonged.
* The above three stages can overlap, and mild cases may not exhibit severe stages.
Methodology
We first searched PubMed, Web of Science, Medline, and Cochrane databases for articles related to SFTS genotype, collected information such as names of DBV virus strains, isolation times, and countries/regions of origin, and downloaded the S segment sequences from GenBank. Based on the downloaded sequences, we conducted phylogenetic analysis, constructed a phylogenetic tree, and validated it.
We used samples obtained from public databases for further validation(to be updated).
Using samples collected from the Sixth People's Hospital of Qingdao and Qishan Hospital in Yantai, we will sequence samples of severe fever with thrombocytopenia syndrome and upload the sequencing results to this website for genotype analysis (to be updated).
Experiment Procedure
Main reagents and materials:Vazyme HiScript II One Step RT-PCR Kit (P611-01), AMPure XP(REFA63881),KAPA Library Quant Kit(Illumina,Universal qPCR Mix,REF07960140001),xGenTM DNA Lib EZ UNI 96rxn(REF10009822),Severe fever with thrombocytopenia syndrome Bunyavirus nucleic acid detection kit (PCR-fluorescent probe method, Daan Gene)
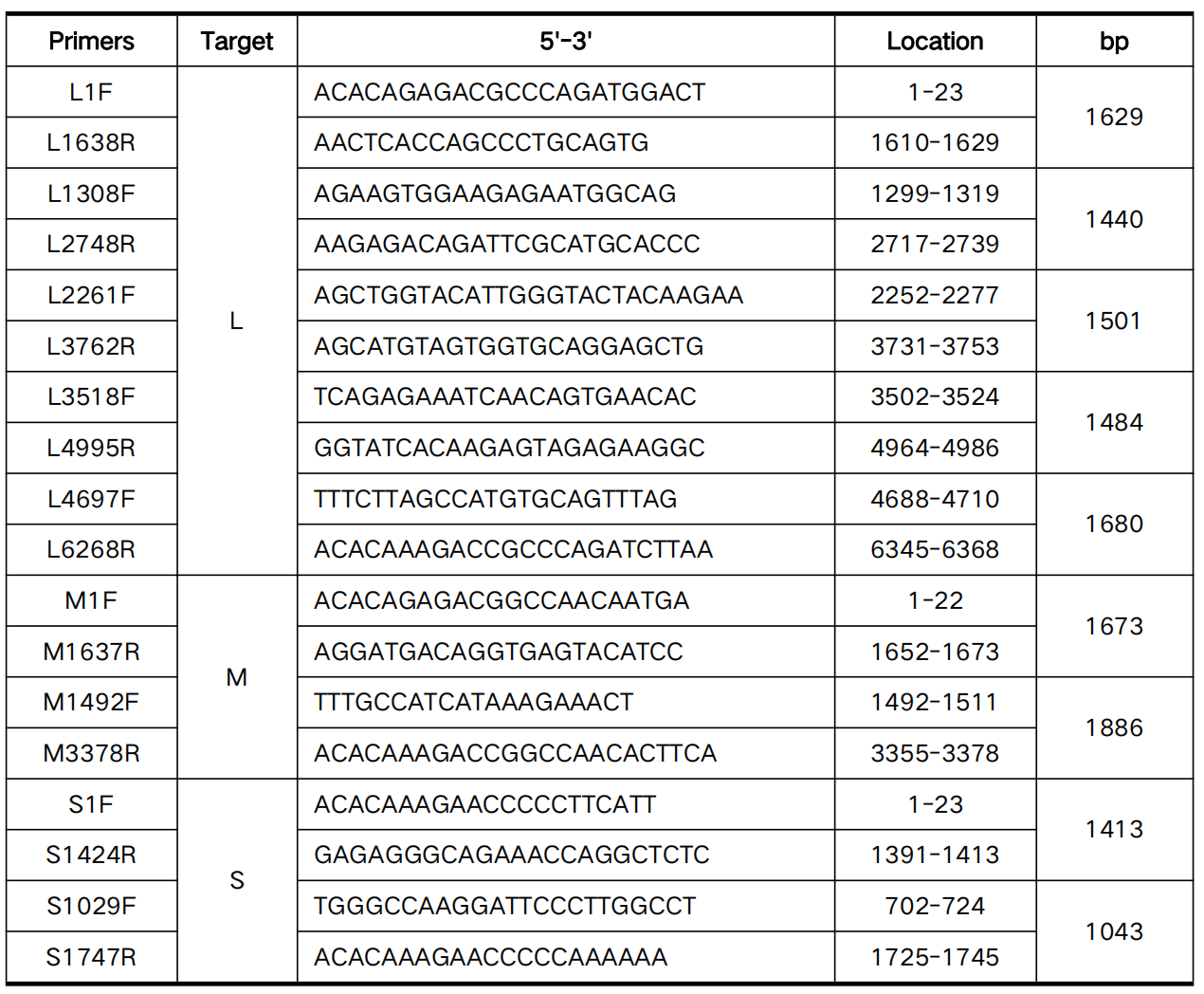
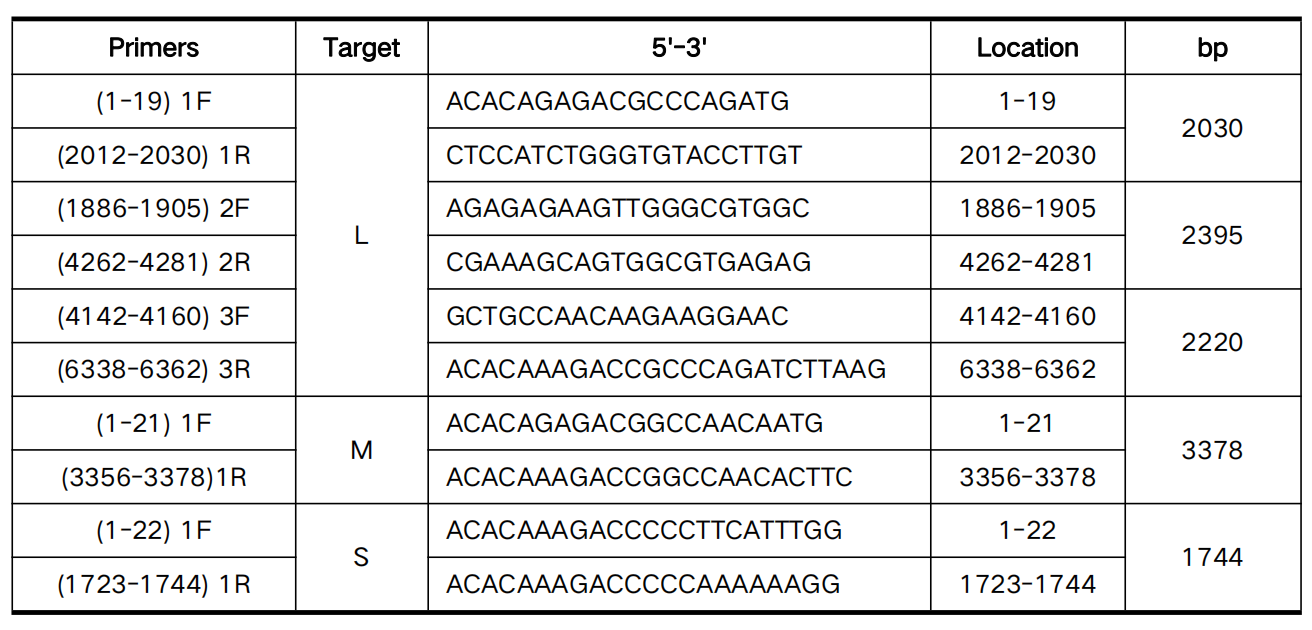
Primers (We used primers mentioned in former articles[4,5])
RT-PCR Reaction Conditions
| Temperature (℃) | Time | Cycles |
|---|---|---|
| 50 | 30 min | 1 |
| 94 | 3 min | 1 |
| 94 | 30 sec | 40 |
| 59 | 30 sec | 40 |
| 72 | 1 min | 40 |
| 72 | 5 min | 1 |
| 12 | ∞ | 1 |
Reference
- [1] Chen QL, Zhu MT, Chen N, Yang D, Yin WW, Mu D, et al. Epidemiological characteristics of severe fever with thtrombocytopenia syndrome in China, 2011-2021. Chinese Journal of Epidemiology. 2022;43(6):852-859.
- [2] Huang XX, Du SS, Li AQ, Li C, Tian TT, Liu TZ, et al. Epidemiological characteristics of severe fever with thrombocytopenia syndrome in China, 2018-2021. Chinese Journal of Epidemiology. 2024;45(1):112-116.
- [3] China NHCotPsRo. Diagnosis and treatment plan for fever with thrombocytopenia syndrome (2023 edition). 2024; http://www.nhc.gov.cn/ylyjs/pqt/202312/75cfff021a484d0c9c200f85f2bf746b/files/39ddd92264f64094985fbef0439da17b.pdf.
- [4] Yun SM, Park SJ, Kim YI, Park SW, Yu MA, Kwon HI, et al. Genetic and pathogenic diversity of severe fever with thrombocytopenia syndrome virus (SFTSV) in South Korea. JCI Insight. 2020;5(2).
- [5] Liu L. Molecular Evolutionary Analysis of Viruses Based on High-throughput Sequencing, Chinese center for disease control and prevention; 2017.